On Monday, March 15th 2021, several European countries, including Germany, halted the AstraZeneca vaccination process following fears linking the occurrence of blood clot-related deaths to the vaccine.
It began when Norway suspended a batch because of seven cases of an extremely rare condition affecting the brain accompanied by a platelet deficiency, an event that manifests itself with spots on the skin (purpura) and an illness that requires hospitalisation.
After that, it was chaos. A similar case happened the next day in Denmark, which also decided to take the same precautionary action. Other countries followed, among them Estonia, Iceland, Latvia and Luxembourg. The European Medicines Agency (EMA) then released a statement announcing they would investigate the cases (therefore encouraging a European response rather than single countries taking action independently).
In Germany, Health Minister Jens Spahn reported another seven suspected cases similar to the Norwegian ones. According to a report from the Paul-Ehrlich-Institut (PEI) , the individuals were 20-50 years old; three of them subsequently died. Six cases were women who had a particular form of cerebral venous thrombosis, while the seventh case was medically very similar (cerebral haemorrhage + platelet deficiency + thrombosis). All cases occurred 4 to 16 days after vaccination with the AstraZeneca vaccine. According to Karl Lauterbach, Social Democrat Spokesperson for Health, the side effects which are the reason the PEI recommended stopping use of the AstraZeneca vaccine occur n one out of 250,000 to 300,000 people who receive the vaccination. According to the PEI, the number of cases following the AstraZeneca vaccination is extremely low but was found to be statistically higher than the number of cerebral venous thromboses that normally occur in the general population (a ratio of 7:1). As a result, the AstraZeneca inoculation was halted as a precautionary measure.
Twitter contribution
On Monday, France, Italy, and Spain followed. Similar decisions had already been taken by other European countries. The question remains as to why these extremely severe cases occurred only in Norway and Germany and none in the UK, where more than 11 million people received the infamous jab? And what does the ‘standard’ thrombosis that all newspapers talked about have to do with the rare conditions found in Norway? Many people, unfortunately, were dying of thrombosis before. Why now this vaccine-related fuss?
From the MedDRA reports (see Pfizer and AstraZeneca links below), it is clear that the number of ‘standard’ thrombosis-related deaths after vaccination equates with the expected number of thrombosis-related deaths under normal conditions. If there was a correlation, then countries where millions of people vaccinated with AstraZeneca would show a marked increase in cases of thrombosis, but there has been no such increase recorded to date (after 10 million vaccinations in the UK, 79 cases of blood clotting, of which 19 fatal). The numbers of thromboembolic events are comparable among those vaccinated with Pfizer and AstraZeneca, the same way they are comparable in the unvaccinated population. As the EMA chairwoman declared on Tuesday, the number of thromboembolic events that occurred during the trial phase among those who received the vaccine were comparable to those that occurred to the people who received a placebo.
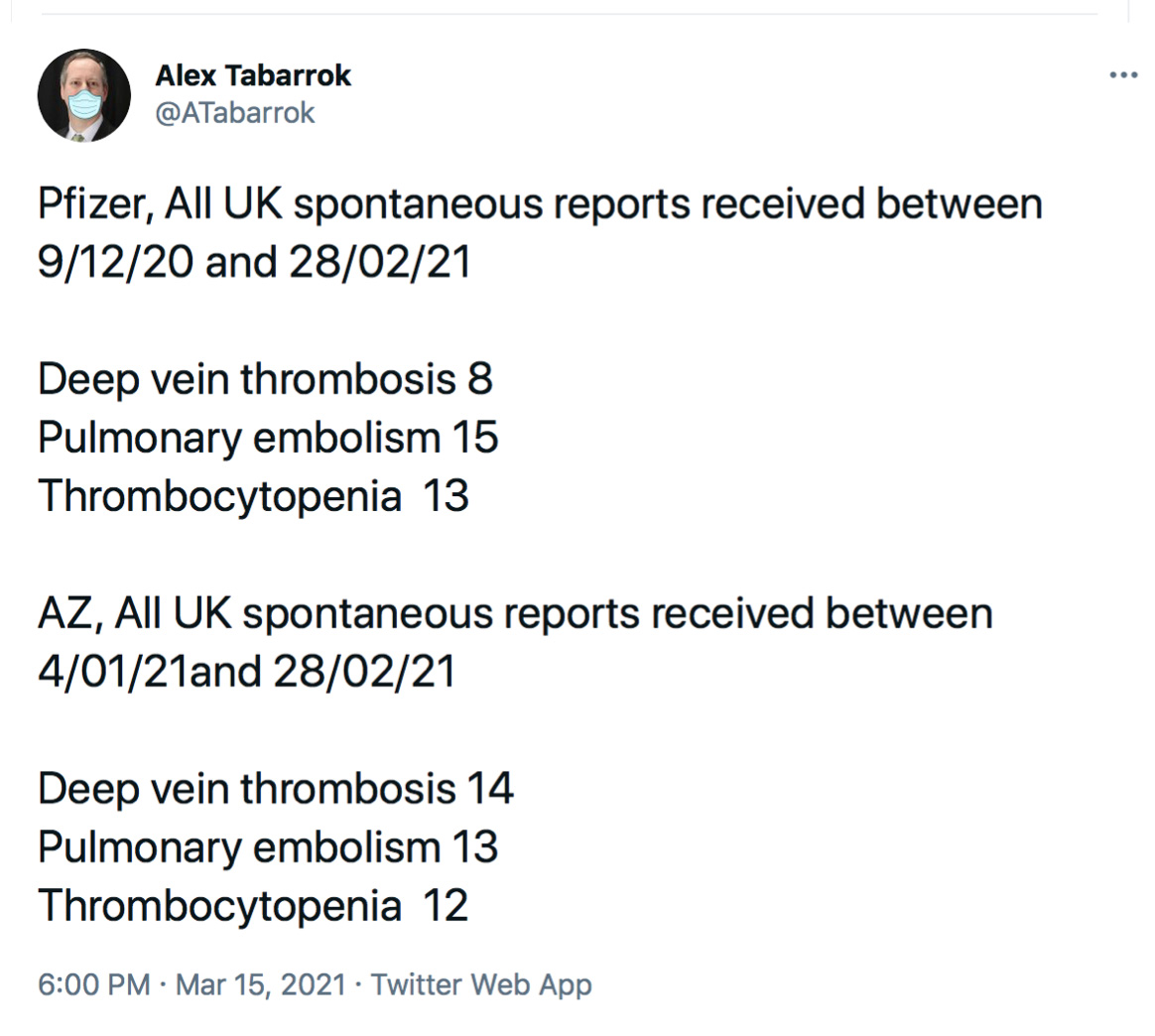
Twitter discussion
The latest update on the EMA website confirms that events involving blood clots, some with unusual features such as low numbers of platelets, have occurred in a very small number of people who received the vaccine. Many thousands of people develop blood clots annually in the EU for different reasons. The number of thromboembolic events overall in vaccinated people does not seem to be higher than that seen in the general population. According to the International Society on Thrombosis and Haemostasis, there are 544,000 VTE (Venous thromboembolism) related deaths every year in Europe alone. That is an average of 1,490 daily. It is then not surprising that some of these include people who may have recently received a vaccination.
In the words of William Shakespeare it seems like a giant case of “much ado about nothing”. A further update will be given by the EMA today, Thursday afternoon, but it is highly likely that the course of action adopted will be similar to that taken so far, namely: the benefits of the vaccine far outweigh its risks, and the AstraZeneca inoculation will resume.
The actual risk, now, beyond the increase in deaths from Covid-19 that this interruption of vaccinations will inevitably bring, is above all a problem of trust. Think about the undecided, the hesitant, the insecure who had reluctantly opted for a vaccine, perhaps convinced by the words of scientists or influencers but who, deep in their hearts, were afraid of the process. They will now think twice (or more) before agreeing to be vaccinated, if at all. The perception of risk associated with vaccines is far greater, not quantifiable with the formulas and percentages we can attribute to thrombosis. It is a perception that seeps into the belly, a feeling of insecurity and fear that stems from the fact that the vaccine might be harmful, now amplified by stories in the media and the response of health departments.
Let’s be honest with ourselves: the risk of contracting Covid-19 is not zero. It is a pandemic. It has reached all corners of the world; even cloistered nuns are affected. Sooner or later, it will reach all of us. What is scarier than Covid-19, though, is the miscommunication around the vaccines. AstraZeneca already had a poor reputation; it was considered the bad guy, the vaccine that doesn’t work so well. When it was cleared for the over-65s, it resulted in a surge of dissatisfaction among older people who somehow felt they had received a vaccine that could not entirely protect them.
And now this. I continue to be very confident in vaccines, including AstraZeneca, convinced that they have been approved because they are safe. I wish there was a Medical Consent Form which I could sign and personally accept the vaccine, rather than having to wait even longer because of delays caused by this media-induced scaremongering.
Why is time so critical in the roll-out of these vaccines? Because if we let Covid-19 spread even further, variants will develop. Some variants may not respond to the vaccines we now have. And then this whole horrendous year will happen again, and again. In just a few months the so called British, Brazilian and South African variants have all appeared.
I’m going to leave you with a small trivia quiz: Which medication has a documented risk of increasing thrombosis affecting 1-10 out of every 10.000 people (many times higher than AstraZeneca)?
Has its use ever been questioned?*
*Hint: it’s a medication for women, not to be taken when ill, but as a precautionary measure. Just like a vaccine.
And do you know what else causes thrombosis? Covid-19.
Sources:
AU https://www.tga.gov.au/alert/astrazeneca-chadox1-s-covid-19-vaccine
AIFA https://www.aifa.gov.it/web/guest/-/aifa-ingiustificato-allarme-sulla-sicurezza-del-vaccino-astrazeneca
UK cases of thrombosis with Pfizer
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/968413/COVID-19_mRNA_Pfizer-_BioNTech_Vaccine_Analysis_Print__2_.pdf
UK cases of thrombosis with AZ
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/968414/COVID-19_AstraZeneca_Vaccine_Analysis_Print.pdf